It is important to use the appropriate CPT codes when seeking reimbursement by payers for covered outpatient procedures, including routine and long-term EEG studies. This article aims to provide guidance on potentially applicable CPT procedure codes for EEG while using Zeto EEG. The details we provide here are informational only, and you should consult your own billing advisors for what is required by your payors. Following this guidance is not a guarantee of coverage or reimbursement.
Billing for Routine EEG
For many reasons, a routine EEG is the most commonly performed EEG study. Choosing the correct CPT Code for routine EEG depends on two factors: how long the EEG is recorded and the patient’s state of consciousness. The EEG billing codes for the applicable time-period are set forth in Table 1.
While procedures with a length of 20-40 minutes require a different code depending on the patient’s level of consciousness, there is a single code for EEGs lasting 41 to 60 minutes, and another single EEG billing CPT code for EEGs lasting greater than 60 minutes, but not in excess of 2 hours. The codes for the longer sessions apply whether the patient is awake, drowsy, asleep, or comatose.
The CPT Code for a 41 to 60-minute routine EEG is 95813 and the code for a routine EEG more than 60 minutes in duration is 95812 (Table 1).
Table 1. CPT Codes for Routine EEG
EEG Length
Clinical Status
CPT Code
Awake and drowsy
95816
20-40 minutes
Awake and asleep
95819
Coma or asleep
95822
41-60 minutes
Awake, drowsy, asleep, or in a coma
95812
>60 minutes
Awake, drowsy, asleep, or in a coma
95813
Other EEG Billing Codes Applicable to Zeto EEG > 2 Hour Recordings
EEG recordings that last longer than 2 hours (“long-term EEG studies”) have their own set of CPT codes. EEGs greater than 2 hours, but less than 12 hours, are billed using the CPT Codes listed in Table 2. Additional CPT codes for EEGs greater than 12 hours are also available but are less applicable for Zeto’s current use case and we have not included them here.
The fact that these EEG billing codes are predicated on the time that the procedure takes makes it imperative that the clinician properly documents the reasons that the particular duration is medically necessary.
Another variable that affects the selection of the correct code for billing the professional component of a long-term EEG monitoring study is whether the EEG is video-recorded. Two EEG “professional component” CPT Codes are available for studies lasting 2 to 12 hours: 95717 is the CPT Code without video, and 95718 is the code with video.
There are also technical component CPT Codes for long-term EEG studies. The CPT Codes for long-term EEG technical components vary based on whether they are unmonitored, monitored intermittently, or monitored continuously.
Table 2. CPT Codes for Long-Term EEG from 2 to 12 hours
Video
Monitoring*
CPT Code Technical Component
CPT Code Professional Component **
Unmonitored
95705
Without Video
Intermittent
95706
95717
Continuous
95707
Unmonitored
95711
With Video
Intermittent
95712
95718
Continuous
95713
* Zeto EEG enables providers to schedule intermittent or continuous EEG monitoring services via third party monitoring providers ** Zeto enables providers to obtain professional EEG reads via third party reading service providers
For individualized guidance on EEG billing, several third-party consulting service providers are active in the market – for questions or an introduction to a consultant familiar with Zeto, complete the form below.
Disclaimer
Zeto, Inc. does not provide billing or coding services and does not offer advice, guidance, or recommendations regarding billing, coding, reimbursement, or claims submission. The information presented in this article is intended solely for general informational purposes and should not be construed as legal, compliance, coding, reimbursement, or financial advice.
It is the sole responsibility of each individual or organization to ensure the accurate selection and application of codes, modifiers, coverage, and documentation, as well as to establish medical necessity and submit claims in full compliance with all applicable federal, state, and local laws, regulations, and payor policies, including those of Medicare, Medicaid, and commercial insurers. To mitigate potential legal, financial, or regulatory risks, it is strongly recommended to consult with qualified legal counsel and experienced coding or reimbursement professionals. Requirements should also be independently verified with relevant payers and authoritative sources, prior to making any billing or coding decisions. This article is not a substitute for professional guidance or independent verification.
Zeto, Inc. makes no representations or warranties regarding the accuracy, completeness, or applicability of the information provided and expressly disclaims any liability for any losses, damages, or other consequences that may result from reliance on this content. Use of this information is at your own risk.
EEGs are an invaluable tool for monitoring real-time brain function at the bedside in the ICU.
Nonconvulsive seizures and nonconvulsive status epilepticus in the ICU are very shockingly common. Now that continuous EEG monitoring (cEEG) has entered clinical practice, we know the incidence of nonconvulsive seizures is between 8% and 37% of ICU patients.1 Up to 22% of patients in the medical ICUwithout brain injury have periodic discharges or seizures.2 Up to 16% of patients in the surgical ICU have seizures.3
Nonconvulsive seizures and nonconvulsive status epilepticus are extremely hard to detect at the ICU bedside—physicians missed 88% of these cases in one retrospective study.4 Sadly, delays in diagnosing and treating nonconvulsive status epilepticus treatment are associated with poor patient outcomes.5,6 Because of this dire need, professional societies and experts are calling on ICU staff to routinely order EEG monitoring in critical care units.7-9
Why order EEG in the ICU?
Seizures and/or status epilepticus causes neuronal damage10 and in some cases, hippocampal atrophy.11 These treatable conditions lead to poor outcomes in both children and adults. Prolonged seizures are associated with chronic cognitive problems and neurological sequelae . In short, undiagnosed and untreated seizures are dangerous for patients.
Making matters worse, seizures are often missed in the ICU setting when the diagnosis is based on clinical signs alone.4 Indeed, as Dr. Lawrence J. Hirsch of the Comprehensive Epilepsy Center of Columbia University in New York put it, “it is fair to say that anyone who works with critically ill neurologic patients and does not see nonconvulsive seizures and nonconvulsive status epilepticus on a regular basis is missing the diagnosis.”12
Given the complex nature of patients’ deficits in the ICU, it is unreasonable to rely on physical/neurological examination alone to detect nonconvulsive seizures.
EEG monitoring does appear to be better able to detect both subclinical seizures and subclinical status epilepticus compared to routine EEG according to a systematic review and meta-analysis study of over 20,000 critically ill adult patients.13
However, this might not translate into long-term clinical benefit, as suggested by a recent multicenter randomized clinical trial in Switzerland called the CERTA study, which evaluated 364 patients using continuous EEG or two routine 20-minute EEGs. The researchers did not find that mortality significantly differed between the two groups at 6 months.
Nevertheless, Neurocritical Care Society guidelines recommend the institution of continuous EEG within an hour of suspecting status epilepticus in all patients.14 Availability of EEG technologists, who can set up a routine and continuous EEGs, play a vital role in enabling ICU EEG monitoring, yet only 26% of institutions have technologists accessible 24/7 in-house.15
According to a study of 625 critically ill patients, preliminary findings from the first minutes of EEG recording have a high predictive value in detecting patients at greater risk for seizures and who would benefit from long-term monitoring.16 The absence of epileptiform discharges after two hours of EEG recording reduced the probability of seizure occurrence to less than 5%, and less than 10% after only 15 minutes.
When to order EEG in the ICU
EEG should be ordered without delay for any ICU patient with suspected nonconvulsive seizures. As mentioned, however, clinical suspicion is not terribly reliable4, thus the bar for ordering cEEG in ICU patients should be very low.
Continuous EEG should be ordered in ICU patients with7,12
Fluctuating mental status
Head trauma
History of convulsive seizures (especially convulsive status epilepticus; about one in two patients with coma and previous convulsive status epilepticus have nonconvulsive seizures.1)
Ischemic stroke
Intraparenchymal hemorrhage
Aneurysmal subarachnoid hemorrhage
CNS infection
Brain tumor
Sepsis
Recent history of ECMO
Hypoxic brain injury of any cause
Continuous EEG monitoring can help critical care physicians properly characterizing “spells” in the ICU “sudden posturing, rigidity, tremors, chewing, agitation, or sudden changes in pulse or blood pressure without an obvious explanation.”12 cEEG can also provide useful information about the level of sedation and can detect clinically silent, but significant neurologic events.12
How to get EEG in the ICU: Rapid EEG Solution
Rapid access to clinical EEGs in ICUs has a significant impact on diagnosis and outcomes in patients with seizures and acute neurological disorders. Despite the obvious need, it is still difficult for most critical care staff to get a rapid EEG in the ICU. The biggest hurdles to EEG in the ICU are a lack of dedicated EEG equipment and full-time staff that can run and read EEG and cEEG studies.
What is Rapid EEG?
EEG performed acutely for new onset of patient events and/or seizures
Designed to be started within a critical time window with the goal of triaging/treating sooner to prevent brain damage
Can be placed quickly by bedside care providers
May be in “screening-quality” category, or may be equivalent to standard EEG quality
How Zeto Can Help
Zeto offers a rapid full montage EEG solution that can be easily deployed in the ICU without a dedicated technologist. Zeto might be used for cEEG for up to 4 hours and for routine EEG. Zeto EEG can provide accurate, high-quality, 19-channel medical-grade EEGs in a matter of minutes (average setup time is about 5 minutes) without skin prep or cleanup.
Virtually anyone who works in the ICU can place the Zeto device with minimal training, it’s possible to use cross-trained personnel. The Zeto team trains onsite and offers remote support.
Once the wireless EEG system is placed on the patient’s head, the resulting EEG is available in real time for live monitoring. ICU staff has the additional paid-on option of real-time remote patient monitoring by registered EEG techs and short-notice remote reads by certified neurologists.
Most importantly, Zeto integrates FDA cleared Seizure Detection and continuous Seizure Load monitoring tools from encevis into its User Interface for automatic detection/notification of such critical events, providing more integrated functionality vs. competitors.
With Zeto, it is now possible to obtain medical-grade EEGs in the ICU setting without an on-site EEG staff. Within minutes, our integrated EEG solution notifies staff of continuous seizures enabling physicians to intervene in a timely manner and save lives in critical care settings.
References
1. Kennedy JD, Gerard EE. Continuous EEG monitoring in the intensive care unit. Curr Neurol Neurosci Rep. 2012;12(4):419-428. 10.1007/s11910-012-0289-0
2. Oddo M, Carrera E, Claassen J, Mayer SA, Hirsch LJ. Continuous electroencephalography in the medical intensive care unit. Crit Care Med. 2009;37(6):2051-2056. 10.1097/CCM.0b013e3181a00604
3. Kurtz P, Gaspard N, Wahl AS, et al. Continuous electroencephalography in a surgical intensive care unit. Intensive Care Med. 2014;40(2):228-234. 10.1007/s00134-013-3149-8
4. Drislane FW, Lopez MR, Blum AS, Schomer DL. Detection and treatment of refractory status epilepticus in the intensive care unit. J Clin Neurophysiol. 2008;25(4):181-186. 10.1097/WNP.0b013e31817be70e
5. Pang T, Hirsch LJ. Treatment of Convulsive and Nonconvulsive Status Epilepticus. Curr Treat Options Neurol. 2005;7(4):247-259. 10.1007/s11940-005-0035-x
6. Trevathan E. Ellen R. Grass Lecture: Rapid EEG analysis for intensive care decisions in status epilepticus. Am J Electroneurodiagnostic Technol. 2006;46(1):4-17.
7. Herman ST, Abend NS, Bleck TP, et al. Consensus statement on continuous EEG in critically ill adults and children, part I: indications. J Clin Neurophysiol. 2015;32(2):87-95. 10.1097/WNP.0000000000000166
8. Herman ST, Abend NS, Bleck TP, et al. Consensus statement on continuous EEG in critically ill adults and children, part II: personnel, technical specifications, and clinical practice. J Clin Neurophysiol. 2015;32(2):96-108. 10.1097/WNP.0000000000000165
9. Rossetti AO, Hirsch LJ, Drislane FW. Nonconvulsive seizures and nonconvulsive status epilepticus in the neuro ICU should or should not be treated aggressively: A debate. Clin Neurophysiol Pract. 2019;4:170-177. 10.1016/j.cnp.2019.07.001
10. Palmio J, Keränen T, Alapirtti T, et al. Elevated serum neuron-specific enolase in patients with temporal lobe epilepsy: A video–EEG study. Epilepsy research. 2008;81(2-3):155-160.
11. Vespa PM, McArthur DL, Xu Y, et al. Nonconvulsive seizures after traumatic brain injury are associated with hippocampal atrophy. Neurology. 2010;75(9):792-798. 10.1212/WNL.0b013e3181f07334
12. Hirsch LJ. Continuous EEG monitoring in the intensive care unit: an overview. J Clin Neurophysiol. 2004;21(5):332-340.
13. Sharma, S., Nunes, M., & Alkhachroum, A. (2022). Adult Critical Care Electroencephalography Monitoring for Seizures: A Narrative Review. Frontiers in Neurology, 13.
14. Brophy, G. M., Bell, R., Claassen, J., Alldredge, B., Bleck, T. P., Glauser, T., … & Vespa, P. M. (2012). Guidelines for the evaluation and management of status epilepticus. Neurocritical care, 17(1), 3-23.
15. Gavvala, J., Abend, N., LaRoche, S., Hahn, C., Herman, S. T., Claassen, J., … & Critical Care EEG Monitoring Research Consortium (CCEMRC). (2014). Continuous EEG monitoring: a survey of neurophysiologists and neurointensivists. Epilepsia, 55(11), 1864-1871.
16. Rubinos, C., Alkhachroum, A., Der-Nigoghossian, C., & Claassen, J. (2020, December). Electroencephalogram monitoring in critical care. In Seminars in neurology (Vol. 40, No. 06, pp. 675-680). Thieme Medical Publishers, Inc.
As with all healthcare professions, neurodiagnostic technologists struggle with staffing shortages, unpredictable situations, and caring for patients with life-threatening physiological disorders. While many healthcare roles have shortages, qualified neurodiagnostic technologists are a rare breed and positions can go unfilled for many months.
In healthcare, there are many things around you that may be out of your control, but you can control how you respond to stressors by being proactive rather than reactive.
Burnout in healthcare workers is very real and is a major concern. Recognize it before it gets worse – people are often so busy that they don’t notice they’re burning themselves out until it’s too late.
We asked Renee DeVere, MS, REEGT, CNIM, Associate Director of Customer Success at Zeto, and an experienced registered EEG technologist to share her recommendations on how to alleviate burnout. She also holds a Masters degree in Industrial-Organizational Psychology.
Self-acceptance
Don’t persecute yourself for what you are experiencing. Burnout is not a weakness, it is a physiological condition.
Take time each day to walk, stretch, and perform relaxing breathing exercises.
Eat healthily and watch your caffeine and alcohol consumption. If you’re drinking a lot of caffeine to keep going and then having an alcoholic drink to reverse it at the end of the day, your physical and mental well-being will suffer. It can be a real rollercoaster and it will affect the quality of your sleep as well.
Compartmentalize your work life from your home life; compassion fatigue is real. Acknowledge when you are feeling it and allow yourself to leave your work behind when you get home. You can have compassion for your patients without living in their shoes. Working in healthcare, you have too many shoes to fill.
Sleep
If your schedule allows you to keep the same bedtime and waketime each day, do it. Switching your sleep schedule all the time causes jet lag. Your mind and body will not perform as well.
If you are on rotating shifts or taking calls, make your sleep a quality one. Darken the room, turn off all electronics before bed, if possible, at least an hour before bed, and create a relaxing bedtime routine and a soothing bedroom environment.
Don’t forget to spend time with supportive friends and family. Share with them, but don’t turn your social time into negativity-binging time. Show others you appreciate them and make time for fun.
Set limits
In healthcare, you can’t control when the stat requests come in, when you get called, when you’re on call, or when your colleagues call in sick and leave you shorthanded, but do learn to set limits wherever possible. Sometimes, if your well-being is on the line, you need to learn when to say no and if it is appropriate to do so. If you empower yourself, you can find the line between essential and excessive.
Be efficient
Look at your workflows, processes, etc. Find out the areas where there is waste, extra steps, overprocessing, etc. Streamline your workflow to reduce redundancy and excess so that each action matters and unnecessary actions are eliminated. Work with your team and team leaders to identify and reduce waste. Promote efficiency by making sure you do not run out of materials needed to do the job and finding additional tools and resources to make work faster or simpler.
For managers of healthcare organizations, ensure that your team members have a voice, respect, and resources needed to perform their roles properly.
Technology Helps
Since 1924 when the first EEG was performed, not much has changed when it comes to picking up the signals from the scalp. Measuring the head, marking electrode locations, scrubbing the skin, applying the conductive paste, gluing down the electrodes, and eventually, tethering the patient to a box with wires – EEG technologists’ jobs involve doing all of these steps again and again.
They spend an average of 20 to 40 minutes just on the set-up. And despite the goal of helping patients, the EEG procedure often makes the patient feel sick.
Modern technology has helped make this process easier in recent years. Today, portable EEG devices offer maximum convenience without compromising the quality of the results. For the EEG techs, these devices reduce prep times (they’re easy to put on and adjust, and there’s no messy glue or wires to clean up), and for the patient, they offer increased comfort (for example, Zeto’s electrode tips are gentle on the skin).
New EEG systems are wireless, portable, easy to use, and cloud-based. Also known as rapid EEGs, these devices make EEG technology much more accessible, allowing more people to benefit from it.
EEG performed acutely for new onset of patient events and/or seizures
Designed to be started within a critical time window with the goal of triaging/treating sooner to prevent brain damage
Can be placed quickly by bedside care providers
May be in “screening-quality” category, or may be equivalent to standard EEG quality
EEGs during COVID times
The pandemic in a way drove innovative change in neurodiagnostics. When COVID initially broke out, many healthcare facilities experienced reduced onsite staffing, and EEG studies were only scheduled on-call by EEG staff. Healthcare worker burnout from COVID reached crisis levels. That’s when registered nurses (RN) started using rapid EEG solutions overnight or for acute needs while onsite EEG staff focused on continuous EEG studies.
After returning to a routine when COVID restrictions lessened, rEEG techniques remained and slowly became a part of the daily workflow at many healthcare facilities. Now RNs and other healthcare providers can perform the setup for acute needs.
Zeto’s Role in Assisting EEG Technologists
Zeto’s mission is to make neurodiagnostics accessible to more patients using the latest technologies. Even though the gold standard in obtaining quality neurodiagnostic recordings is to deploy a registered EEG technologist, there is an undeniable shortage of them in the US.
According to statistics, there were a mere 6,500 EEG technologists in 2018, with a likely need of 30,000. Throughout the pandemic, the need for EEG technologists has further increased. We believe that Zeto can help fill this gap by providing time-saving innovations with remarkable simplicity.
The Zeto team sees every day how their technology enhances EEG tech work. Modern EEG technology cannot replace EEG technologists, but it can make their job easier and less burdensome. For example, the Zeto setup process generally takes less than 5 minutes, and it is also convenient for patients because no skin preparation is required and no gel is used. Zeto allows technologists to focus on the most important parts of the EEG study – obtaining quality EEG data, scanning EEG patterns, and alerting neurologists as soon as possible when needed.
“In addition to assisting EEG technologists, wealso see a tremendous value of Zeto during triage situations where clinical necessity requires immediate neurodiagnostic testing. In many acute settings, EEG technologists aren’t physically able to arrive soon enough, and ‘time is brain’ for the patient.
In these situations, any trained healthcare professional, such as a nurse, medical assistant, or respiratory specialist, can hook up the patient using Zeto. During recording, it is necessary to know what a high-quality EEG should look like. This is where Zeto’s cloud platform becomes essential. Remotely, using a simple video tool, neurodiagnostic technologists can monitor the EEG in real-time to validate the EEG’s studies quality.
In situations where in-house registered EEG technologists are unavailable, Zeto is partnering with accredited monitoring services that provide live remote video monitoring at an hourly flat rate.
Zeto headsets can bridge the gap until more traditional EEG recordings by registered EEG technologists become available. In the past two years, we saw multiple examples of how Zeto technology helped support providers by making EEGs more accessible even under the most challenging circumstances,” said Florian Strelzyk, Chief Sales Officer at Zeto.
The Electroencephalogram (EEG) can be used as a Biomarker for Dementia. This decades-old technology is finding new life in modern neuroscience.
Old Dog
Introduced to neurologists for the detection and classification of epilepsy by Frederick Gibbs’ in 1934, electroencephalography (EEG) has played an integral role in the history of neurological medicine.
Not even the introduction of Computed Tomography (CT), Magnetic Resonance Imaging (MRI), magnetoencephalography (MEG), and other neuroimaging technologies could replace EEG as a low-cost, noninvasive tool for evaluating cortical function.
Presently, the role of EEG remains limited by the relatively low spatial resolution. However, the superior temporal resolution made EEG an indispensable device in clinical neurology. EEG reading physicians with trained eyes can interpret subtle deviations of electrographic signals from normal brain activity. However, oftentimes these electrographic events cooccur with overt behavioral symptoms that seem to render EEG unnecessary. Nevertheless, these behavioral manifestations can be misleading. For instance, classifying psychogenic seizures, which do not have underlying abnormal brain activity, from epileptic seizures is primary importance for the subsequent treatment plan of the patient. This distinction can only be possible based on EEG evidence or the lack thereof.
Even so, interest in EEG has exploded over the last two decades. The recent leaps forward in computing power and advancements in machine learning have begun to change the practice of medicine. In neuroscience, attention has turned toward overcoming the limitation of the poor spatial resolution of EEG.
There are two streams of advancements in EEG data augmentation and analysis. One is to improve source localization and the other is to utilize the EEG to find biomarkers of diseases using Machine-learning algorithms. What makes the latter approach viable today is the aggregation of large amounts of EEG data on a scale previously impossible. The special characteristics that have kept EEG relevant for so long – non-invasive and inexpensive – have become even more compelling.
New Tricks
The first practical applications for these augmented EEG data examinations will most likely involve using EEG to locate biomarkers–tools to facilitate the early diagnosis of diseases, dementias especially. A biomarker is a piece of measurable and objective biological data used to diagnose or stage an illness. Presently, the most frequently used EEG detectible dementia-related biomarkers include those used to identify Alzheimer’s disease (AD).
Alzheimer’s disease biomarkers, identified using EEG, improve the objectivity to the detection and prognosis of AD. That objectivity can provide the much-needed confidence for physicians, and presentable evidence to the patients and families under evaluation. Researchers classify AD biomarkers in the following categories:
Biochemical,
Radiologic,
Genetic,
Neurophysiological.
Both biochemical and radiologic biomarkers have found their way onto AD diagnostic criteria.
Biochemical markers incorporated in AD work-ups include CSF analysis checking for the presence of amyloid, total tau, and hyperphosphorylation tau proteins. AD diagnostic evaluations frequently include radiologic biomarkers such as the atrophic findings on structural MRI or metabolic changes on fluorodeoxyglucose (FDG)-PET. Genetic markers have yet to merit inclusion as independent AD criteria. Genetic biomarkers, especially those focused on specific alleles of apolipoprotein E, have shown some promise as supporting markers.
Computer augmented EEG data techniques have been the focus of research attempting to establish neurophysiological biomarkers to add a function-based evaluation to AD diagnosis. Leveraging increased computing power has allowed denoising, improved localization, and non-linear analysis. These advanced EEG techniques now assist in Alzheimer’s disease and dementia diagnosis during preclinical stages. Candidates for EEG-derived biomarkers of Alzheimer’s disease include both linear-spectral and non-linear dynamic features. Linear features of AD typically include:
Slowing of alpha power,
Increase in delta power,
Theta power is higher in patients with vascular dementia compared to AD,
Zero crossing interval (ZCI) increased in slow activity associated with dementia.
The work of laying the foundation for EEG biomarkers in the diagnosis of Alzheimer’s disease and dementia continues. Neuroscientists continue decoding how functional changes in the dementia-impacted brain reveal themselves in EEG data. The list of EEG biomarkers will narrow and expand as our understanding improves. Ultimately, EEG biomarkers will sharpen our ability to diagnose and triage different types of dementia at an earlier phase of the disease than we do today. Utilizing EEG to detect early markers for Alzheimer’s disease and dementias may open the door to new therapeutic possibilities or create the opportunity for patients and their families to plan ahead. For diligent neurologists, the ongoing pursuit of EEG biomarkers will require sustained attention. The future has begun to arrive.
The Covid-19 pandemic has had negative effects on the health and well-being of many individuals around the world, often leaving persistent decreases in quality of life in the post-acute phase of illness. Studies of survivors across the globe, including the United Kingdom, Spain, the United States, and France found lasting neurological effects from Covid 19in thirty percent or more of study subjects when they were followed up after hospital discharge.¹
How does Covid 19 affect the brain?
In terms of how Covid 19 affects the brain, symptoms not only included fatigue and dyspnea, but also neuropsychiatric maladies, such as post-traumatic stress disorder (PTSD), anxiety, depression, and concentration and sleep abnormalities.¹ A prospective cohort study out of Wuhan, China showed similar results. Fatigue/muscular weakness (63%), followed by sleep disturbance (26%) and anxiety/depression (23%) were the most frequent lingering symptoms. Beyond effects on mood and energy, features of Covid-19 infection show that it can affect the brain and central nervous system, including loss of sense of smell and taste, concentration deficits, and headache.² At its most extreme, symptoms can include encephalopathy and seizure.
Source: Shutterstock
EEG Neurofeedback
EEG neurofeedback is a promising technique to provide clinical benefit to those suffering from neuropsychiatric complaints as an alternative or complementary therapeutic modality to conventional psychopharmacology, which carries the risk of many undesirable side effects.
The International Society for Neuroregulation and Research explains the EEG neurofeedback process. They say, “During training, sensors are placed on the scalp and then connected to sensitive electronics and computer software that detect, amplify, and record specific brain activity. Resulting information is fed back to the trainee virtually instantaneously with the conceptual understanding that changes in the feedback signal indicate whether or not the trainee’s brain activity is within the designated range. Based on this feedback, various principles of learning, and practitioner guidance, changes in brain patterns occur and are associated with positive changes in physical, emotional, and cognitive states.”
A review article by Sharon Niv discusses this potential for a variety of disorders, including ADHD, autism spectrum disorders, substance use, PTSD, depression, sleep disturbance, and learning disabilities.³ Although most of these studies were not well-designed and placebo-controlled, the majority suggested clinical benefit.
A recent study by Ward, Porter, and Wood showed outpatient EEG neurofeedback reduced neuropsychiatric complaints, including hyperactivity, emotional lability, anxiety, and depression symptoms.4 Research by Escolano et al. demonstrated that neurofeedback could be effectively employed to enhance cognitive function (specifically working memory) that is negatively impacted by major depressive disorder (MDD).5 The benefit of neurofeedback in the setting of depression may be augmented by photic stimulation.6
Source: Shutterstock
EEG and Covid 19
An article by Kopańska et al. reviewed the most recent research on EEG findings in patients with COVID-19, including 17 publications in their evaluation.2 One pattern they identified was that changes frequently involved the frontal area of the brain, which controls focus and executive function. A nonspecific encephalopathic pattern was commonly found, although this pattern could be distinguished from infectious toxic encephalopathy or post-cardiorespiratory arrest encephalopathy using quantitative EEG (qEEG).7 Epileptic discharges and frank seizures or even status epilepticus were detected in a relatively small number of affected individuals.8 The degree of abnormality was associated with Covid severity and pre-existing neurologic disease.
Abnormal EEG patterns identified in patients with Covid-19 are potential targets for EEG neurofeedback. Luckos, Cielebak, and Kaminski published a case study on the therapeutic potential of this modality specifically for Covid.9 A 48-year-old woman developed neurocognitive deficits described as “brain fog” about a month after contracting Covid-19 infection. Her decline was so severe that she was no longer able to function independently.
EEG neurofeedback coupled with goal-directed cognitive training behavioral training was able to greatly alleviate her symptoms, and she was able to resume work. Others affected by Covid’s lasting neurological effects might similarly benefit.
It seems clear that Covid 19 impacts the brain, and that Covid causes lasting neurological effects. It seems equally clear that EEG neurofeedback may be a big help to those who have had Covid 19.
References
1. Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, Cook JR, Nordvig AS, Shalev D, Sehrawat TS, Ahluwalia N. Post-acute COVID-19 syndrome. Nature medicine. 2021 Apr;27(4):601-15.
2. Kopańska M, Banaś-Ząbczyk A, Łagowska A, Kuduk B, Szczygielski J. Changes in EEG recordings in COVID-19 patients as a basis for more accurate QEEG diagnostics and EEG neurofeedback therapy: a systematic review. Journal of clinical medicine. 2021 Jan;10(6):1300.
3. Niv S. Clinical efficacy and potential mechanisms of neurofeedback. Personality and Individual Differences. 2013 Apr 1;54(6):676-86.
4. Ward KP, Porter NA, Wood DS. The effectiveness of neurofeedback in an outpatient setting: A multilevel modeling approach. Research on Social Work Practice. 2019 Nov;29(8):939-48.
5. Escolano C, Navarro-Gil M, Garcia-Campayo J, Congedo M, De Ridder D, Minguez J. A controlled study on the cognitive effect of alpha neurofeedback training in patients with major depressive disorder. Frontiers in behavioral neuroscience. 2014 Sep 2;8:296.
6. Hammond DC. Neurofeedback treatment of depression with the Roshi. Journal of Neurotherapy. 2000 Jun 1;4(2):45-56.
7. Pastor J, Vega-Zelaya L, Martin Abad E. Specific EEG encephalopathy pattern in SARS-CoV-2 patients. Journal of Clinical Medicine. 2020 May;9(5):1545.
8. Antony AR, Haneef Z. Systematic review of EEG findings in 617 patients diagnosed with COVID-19. Seizure. 2020 Dec 1;83:234-41.
9. Luckos M, Cielebak K, Kaminski P. EEG NEUROFEEDBACK IN THE TREATMENT OF COGNITIVE DYSFUNCTIONS AFTER THE INFECTION OF SARS-CoV-2 AND LONG COVID-19. Acta Neuropsychologica. 2021:361-72.
People with epilepsy typically experience recurrent seizures. Despite the diverse causes of seizures, the common mechanism linking many types of epilepsy is the disruption of the brain’s normal electrical activity, which temporarily halts communication between neurons.
About 60% of epilepsy cases have a cause, a lesion, or abnormality in the brain, detectable by neuroimaging methods [1,2]. Another class of pathogenesis of numerous epileptic symptoms is an abnormal expression of specific receptors in the brain, which leads to increased excitation and decreased inhibition resulting in enhanced neural activity.
Because epilepsy can only be diagnosed based on electrophysiological evidence (detection of two independent epileptic events by EEG tests) the use of EEG is mandatory for epilepsy diagnosis and management. Furthermore, based on the EEG evidence a trained epileptologist can determine the type of seizure and diagnose the type of epilepsy syndrome of the patients. The exact diagnosis can help to provide effective antiepileptic medication and prognosis.
Let’s find out the role of EEG in diagnosis, classification, and management in more detail. But first, let’s discuss what an EEG is.
What is EEG?
Electroencephalogram (EEG) is non-invasive research and diagnostic tool used to measure the changes of the brain’s electric potential over time, commonly called brain waves. This electric potential is generated by the discharges of millions of neurons. Although EEG does not have the spatial resolution of detecting the discharges of individual neurons, it can discern levels of activity associated with the major lobes of the human cerebral cortex. In other words, the EEG is a test that helps to detect electrical activity and abnormalities in a patients’ brain and localize them with a certain precision sufficient to make a diagnosis. An EEG equipment uses small sensors (electrodes) made of a conductive material attached to the scalp or they contact the skin. Often these electrodes are preconfigured inside an EEG headset to speed up the positioning.
Typically, specialists, clinical neurophysiologists, neurologists, and researchers carry out an EEG recording. Traditionally it has been done in clinics or academic laboratories and also has been adapted for home monitoring. While EEG has numerous research applications from basic research to Brain-Computer-Interface (BCI), in the field of clinical neurology it is mainly used to diagnose and monitor epilepsy and sleep disorders.
Diagnosis, Classification, and Patient Management
Diagnosis and treatment of epilepsy are often challenging. However, modern therapy provides many patients with multiple treatment options and often complete control of the seizure. After the first two seizures, evaluation should concentrate on:
1. Ruling out any non-epileptic medical or neurological condition that may generate seizures (e.g., psychogenic seizures)
2. Determine the type and location of seizures (e.g., focal, generalized, convulsive, non-convulsive)
3. Evaluating the relative risk of a seizure episode
4. Evaluating treatment options (e.g., diet, pharmacological treatment, surgical intervention, implanted control device)
The Use of EEG in Diagnosis of Epilepsy
Regardless of technological advancements, the first seizure episode typically is not captured in EEG. Numerous paroxysmal events can be confused with epileptic seizures, such as movement disorders, syncope, psychogenic seizures, etc. Probably, the most common event confused with epileptic seizures is syncope. To rule out non-epileptic seizures one needs to record abnormal activity from the brain as primary evidence. This is done by EEG equipment because all other methods to record brain activity are more expensive. At the same time, it is generally recommended to carry out a brain imaging study, such as magnetic resonance imaging (MRI). The MRI can reveal underlying cerebral lesions such as a tumor, stroke, vascular malformation, that could explain the seizure and also help localize it. However, not all epileptic seizures are associated with morphological differences in the brain that can be resolved by MRI. The class of epilepsy associated with electrographic seizures without visually observed MRI evidence is called non-lesional epilepsy.
The Vital Role of EEG in Epilepsy Diagnosis
Why does EEG play a central role in epilepsy diagnosis and treatment? Because EEG can:
● detect epileptiform activity,
● strengthen the putative diagnosis,
● identify the focal cerebral abnormalities, which may indicate a focal structural anomaly such as brain tumor, hemorrhage, vascular malformation and
● document particular epileptiform activity patterns linked to specific epilepsy syndromes
Trained clinicians can recognize a particular type of epilepsy based on their signature waveforms and distribution using an EEG device. Each type of epilepsy diagnosis entails specific treatment strategies. Typical EEG results provide a multiaxial diagnosis of epilepsy describing whether the seizure disorder is generalized or focal, symptomatic or idiopathic (unknown cause), or part of a particular epilepsy syndrome. Because no two epilepsy cases are identical, providing a detailed description of the type of epileptic waveforms, the topography (location in the brain), the frequency of occurrences, the triggering stimulus if there is any, and the effect of seizure on the cognitive and motor functions are all important aspects shaping the treatment strategy.
One critical aspect of epileptic seizures that can be captured by an EEG study is whether it is generalized or focal. The two require completely different medication and treatment strategies. In the case of generalized seizures, abnormal synchronized discharges quickly spread to both cerebral hemispheres, while in focal seizures the abnormal discharges remain localized to a certain area or areas. To capture these events, one needs to spend hours or days with a continuously recording EEG because these events are rare unless it is triggered by a known stimulus (light, sound, touch, anxiety, hyperventilation, etc.).
Because of the scarcity and unpredictable nature of epileptic seizures, these events may not be captured in the clinic during the EEG. However, the description of a seizure by a witness combined with the patient’s self-report can complement the information available from EEG. Abnormal EEG activity patterns that indicate the potential for seizures are called inter-ictal events (sharp waves and spike and waves). These events play an important role in localizing and seizures. Today, a lot of attention is paid to interictal events as potential biomarkers of an impending seizure. One of the biggest machine learning challenges in medicine is to predict seizures based on the types and occurrences of these interictal events.
The role of EEG in Classification of Epilepsy
The classification of epilepsy and the recognition of diagnostic categories based on EEG is an ongoing, evolving process. The categories we use today are not the same as the ones we used 30 years ago, and they change as we understand the disease better. We tend to overclassify epilepsy syndromes as each is associated with particular EEG features. Therefore, it is the task of an internationally elected committee of experts ”International League Against Epilepsy (ILAE” to update the classification systems from time to time, based on consensus and published empirical evidence [3]. Because the classification is evidence-based, and evidence is subject to technological advances, the EEG and other methods, such as neuroimaging, molecular biology, and genomics have a great impact on the classification progress. And will be informed as times go on by developments in imaging, molecular biology, and genetics.
The role of EEG in Management of Epilepsy
The main objective for treating epilepsy patients is to control seizures entirely without causing undesirable side effects. Therefore, besides EEG being an indispensable part of diagnosis, it is also necessary for epilepsy management. Until today the primary measure of the efficacy of epileptic drugs was the extent it reduces seizure frequency. This assessment was often based on self-reports, diary, and caretakers’ notes. With the widespread availability of EEG, this is expected to change and EEG could be utilized for quantifying the efficacy of any treatment, from drug therapy to special diets.
Conclusions
Patients diagnosed with epilepsy have more therapeutic options available to them today than yesterday. To maximize the benefit of these options, clinicians must make an accurate diagnosis of epilepsy syndrome, select and use medications effectively, and promptly refer patients where necessary.
Among the broad range of available diagnostic methods, EEG is still the most versatile and affordable research and diagnostic tool that helps study the brain’s electrical activity and recognize patterns associated with epilepsy. Most importantly EEG provides detailed information about the type and localization of epilepsy.
While it has a very limited spatial resolution and is prone to misinterpretation, EEG remains the gold standard of epilepsy diagnosis. It is and it will remain in the equation to provide better care for patients and to feed our curiosity about the inner workings and communications of brain tissue.
References:
1. Nguyen DK, Mbacfou MT, Nguyen DB, Lassonde M. Prevalence of nonlesional focal epilepsy in an adult epilepsy clinic. Can J Neurol Sci. 2013 Mar;40(2):198-202. doi: 10.1017/s0317167100013731. PMID: 23419568.
2. Téllez-Zenteno JF, Hernández Ronquillo L, Moien-Afshari F, Wiebe S. Surgical outcomes in lesional and non-lesional epilepsy: a systematic review and meta-analysis. Epilepsy Res. 2010 May;89(2-3):310-8. doi: 10.1016/j.eplepsyres.2010.02.007. Epub 2010 Mar 15. PMID: 20227852.
3. https://www.ilae.org/guidelines/definition-and-classification/proposed-classification-and-definition-of-epilepsy-syndromes
When the British physician Richard Caton first recorded the brain’s electrical activity on a rabbit in the late 19th century he didn’t know his groundbreaking experiment would inspire the invention of a line of revolutionary technologies that turned out to be indispensable assets of neuroscience. One of those inventions is Hans Berger’s electroencephalography (EEG), which transformed the diagnosis of neurological conditions. Since then EEG has gone through several advancements, of which a key one is active EEG electrodes.
Because every innovation comes with certain pluses and minuses, it is of primary importance to clarify them for users. The guiding principle of any EEG innovation is to improve the quality of signals recorded from the brain while balancing usability and user comfort. Only after fully understanding these pros and cons could one make the right choices for their use case be it clinical, research, or other.
What are Active and Passive Electrodes?
The brain’s electrical activity (brain potential) is a sum of the myriad discharges generated from neuronal action potentials. Although a single action potential is detectable in the millivolt (mV) range, the combined effect of a large population of neurons on the voltage of the brain tissue relative to a neutral point is the sum of all action potentials. Because of the inherent stochasticity of these action potentials, the simultaneous positive and negative fluctuations cancel each other. Therefore, the net voltage fluctuation in the brain tissue is a fraction of that of the neuron, yielding to a fluctuation in the microvolt (uV) range. Fortunately, neurons often act in concert to achieve effective control of target tissues. When they do so, the millions of action potentials synchronize in oscillatory patterns like flocking birds synchronize their flying. Those oscillations form traveling waves over the surface of the cerebral cortex penetrating the skull and yielding to discernable voltage fluctuation over the scalp, a signal known as EEG.
To noninvasively capture the brain’s electric potential fluctuations over the skull, two different EEG electrode technology options are available. One is passive electrodes and the other is active electrode technology. Passive electrodes are traditional EEG electrodes that simply transmit the voltage fluctuation to the amplifier through a conductive wire. To attain a low-impedance contact we use Silver-Silver Chloride (Ag/AgCl), or gold electrodes. However, the need for skin preparation to achieve a low enough impedance (under 10Kohm), the cost of the electrodes (~$10/electrode), the labor-intensive gluing method, the inconvenience to the patient, and most importantly the increasing cases of skin breakdown encouraged innovation in EEG electrode technology. A well glued gold-cup EEG electrode on a clean exposed skin surface with an adequate amount of electrode paste on a relaxed motionless subject in an electromagnetically shielded room, with the amplifier a few feet (1-2 m) distance from the subject, can provide a relatively clean EEG, that shows discernible delta, theta, alpha, beta oscillations in the EEG. These oscillations originate from the brain, hence passive electrode technology was for a while the ultimate low-cost, noninvasive brain activity monitoring modality for extensive clinical and research purposes.
Active electrode technology was developed partly in response to not needing skin preparation. The second factor was to prevent the weak EEG signal from being contaminated by noise while traveling through the long wire. The solution to handle both was moving a part of the amplifier as close as possible to the electrode thereby buffering the signal close to the scalp (Fig. 1). Because in the case of active electrode implementation the cables carry a signal driven strongly by the pre-amplifier which makes it less susceptible to electromagnetic interference thereby improving the signal to noise ratio. A high input impedance pre-amplifier also mitigates the need for abrading skin or using conductive paste in order to drop skin impedance.
Figure 1. The graphical scheme of conventional EEG with an instrumentation amplifier before the backend (a) versus the active electrode solution where the amplifiers are placed proximal to the electrodes (From Xu et al., 2017).
The Active electrode has two components, the electrode, and the preamplifier circuit. The electrode materials need to be carefully chosen so as to not have polarization effects and are typically silver/silver chloride (Ag-AgCl). The performance of such a dry-active electrode array was first demonstrated at the University of California, Davis, by Babak Taheri in the 1990s.
Passive electrodes, in contrast, are generally plated with Ag-AgCl or gold and need electrolytic paste or gel (they are frequently called wet electrodes for this reason). However, the scalp is first prepared to minimize electrode-scalp impedance which is recommended to be under 10Kohm.
A report of the construction, performance, and results of the first dry-active electrode appeared in a 1994 scientific publication. One of the initial observations made was the fact that the arrayed active electrodes outperformed the passive electrodes.
To understand how active electrodes could achieve such a good performance we need to compare the underlying signal transmissions implemented by these two types of EEG electrodes.
Pros And Cons of Active and Passive EEG Electrodes
Active and Passive Electrodes Pros
Active electrodes allow pre-amplification modules close to the electrode. Hence, these EEG electrodes enable signal amplification before any extra noise attacks the EEG signal.
Active electrodes can make a big difference in a multitude of scenarios. First and most important, they enable the use of dry electrodes. Dry electrodes, in general, are associated with higher noise levels because they are not glued to the skin surface nor do they use a conductive gel that creates a low impedance bridge between the skin and the EEG electrodes.
Likewise, active electrodes do great when the measurement occurs in areas with fair amounts of electromagnetic noise and when there will be a considerable distance between the system and the electrodes used for EEG.
For passive electrodes, a conductive gel is a must to minimize impedance, so as to enable the signal to travel reliably through the wire. Moreover, during extended usage of wet passive electrodes, the gel may dry up leading to poor quality of the recording.
Active and Passive Electrodes Cons
On the other hand, passive electrodes are simpler to manufacture, and they cost and weigh less as they lack the pre-amplification modules that active electrodes have. Active electrodes also require more wires (additional power and ground) to enable the functioning of the pre-amplifier. Passive electrodes can achieve very good performance when the electrode has a stable low impedance.
Comparing Active and Passive EEG Electrodes in Amplification System Test
A growing number of studies demonstrated a superior signal quality of active electrodes over passive electrodes. When the active electrode technology is applied to dry electrodes, it can compensate for the higher impedance of the dry electrodes and achieve equivalence with the gel-loaded passive electrodes with all the benefits deriving from the active electrodes.
The illustration below was taken from a study involving 8 participants after recording EEG reading following the emission of auditory stimuli.
The reading produced by the active electrodes was instantaneous in response to the Event-Related Potentials (ERPs) recorded after the emission of the auditory stimulus. Furthermore, there was a significantly reduced error in the voltage difference between the EEG electrodes’ recorded measurement and the reference signal.
Another study compared the active and passive electrodes in an ERP during cognitive tasks (Laszlo et al., 2014). The study involved two experiments. In the first experiment, researchers manipulated interelectrode impedance in an electrically quiet setting to check if active electrodes produced better results under such recording conditions. In the second experiment, they studied active electrodes’ ability to record when limited by natural skin impedance. The investigation also explored the relationship between voltage stability and active amplification circuitry in EOG. Results from both experiments showed complicated connections between voltage stability, electrode types, and impedance. Ultimately, the study indicated that active electrodes outperformed passive electrodes at different impedance levels except for very low ones. To be specific, passive electrodes obtained higher quality data only when impedance was less than 2 kΩ. That said, it’s worth noting that passive ones also were better at accurately following the EEG than active ones in the event of rapid voltage fluctuations.
Conclusion
The quality of EEG recordings depends on several factors. Whether you prefer to use an active electrode EEG system or not, it is vital to know the pluses and minuses. Active electrode technology when used with high-quality electrodes (e.g., gold-plated) with conductive paste provides the best of both worlds, i.e., low skin impedance and a well-driven signal that is less susceptible to noise. However, in such cases when these electrode wires need to be disposed of due to wear and tear along with the pre-amplifier assembly, the cost could become prohibitively expensive. Hence active electrodes most commonly enable the use of dry electrode EEG systems, which allows you to reuse the EEG cap and dispose of just the electrodes. Such wireless EEG systems also enable the fast and easy setup of EEG without elaborate prep work. Signal quality in such cases has shown to be as good or in some cases better than just conventional passive electrodes. In summary, active electrode technology always makes the EEG signal quality better. They cost more because of the additional circuitry and wires needed. If disposed of with the electrode wires, they could be too expensive; however, if reused with a cap-like system, the cost is not a concern. With costs dropping fast for such commodity parts, there is adequate reason to believe active electrodes will replace passive ones in the next few years.
REFERENCES:
1) Xu J, Mitra S, Van Hoof C, Yazicioglu RF, Makinwa KAA. Active Electrodes for Wearable EEG Acquisition: Review and Electronics Design Methodology. IEEE Reviews in Biomedical Engineering. 2017 ;10:187-198. DOI: 10.1109/rbme.2017.2656388.
2) Kelly, J. W., Siewiorek, D. P., Smailagic, A., & Wang, W. (2013). Automated filtering of common-mode artifacts in multichannel physiological recordings. IEEE transactions on bio-medical engineering, 60(10), 2760-2770. https://doi.org/10.1109/TBME.2013.2264722
3) Laszlo S, Ruiz-Blondet M, Khalifian N, Chu F, Jin Z, A direct comparison of active and passive amplification electrodes in the same amplifier system, Journal of Neuroscience Methods, 2014, Volume 235, 298-307, https://doi.org/10.1016/j.jneumeth.2014.05.012.
The dry electrode EEG system is a new development in the field of diagnostic science, offering an alternative to the conventional wet electrode EEG system.
To replace the wet EEG setup in clinical settings, dry electrode headsets must convey high-quality signals and give accurate results in terms of latency and amplitude. The dry electrode systems must also be able to separate biological signals from background noise.
Before comparing these two approaches, it is important to understand how each one of them works.
A brief overview of the wet EEG device
The traditional EEG system consists of small metal discs (electrodes), covered with a silver/silver-chloride coating, which are placed on the scalp. Some recording systems use elastic head caps, which have electrodes built-in in preset positions, expediting the correct electrode placement according to the 10-20 international standard, assuming a proportional expansion and distribution of electrodes over different head sizes.
Other, more traditional approaches, place single leads on the scalp one at a time using glue, gauze, and tape. An electrode gel is applied to the skin under the electrode to improve the skin-electrode conductivity and to reduce impedance. It also decreases the artifacts produced by the movements of electrode cables.
Once the electrodes are positioned, it often requires scraping the surface of the skin using various tools to remove the upper layer of skin to improve the conductivity between the skin and the gel.
Then the electrode is ready for recording the brain’s electrical activity and analyzing the data for diagnostic purposes.
A brief overview of the dry EEG device
In contrast to traditional electrodes, dry EEG systems make contact directly with the scalp and do not require conductive gel to be applied between the skin and electrode. That is made possible because of additional system components that increase the EEG signal strength right at the scalp.
Since they do not require any skin preparation, dry electrodes make the EEG headset suitable for rapid EEG tests, eventually, beyond healthcare facilities. The dry electrodes are easy to place without the help of any additional instruments like syringes or gel cans.
Moreover, after use, there is no need to clean the head as dry electrodes leave no residue on the skin or on the hair. Because dry electrodes are often made of plastic, they are affordable and can be made disposable, hence their use is a lot more hygienic and safer to be transferred between patients than traditional multiple-use electrodes.
Comparison of the dry and wet EEG system
The main purpose of introducing dry electrodes to be used in EEG systems was to improve the comfort of patients and experimental subjects while reducing the time of preparation. The dry electrodes are cleaner, more comfortable, quicker to set up and quicker to remove. In short, they are more practical.
In addition to convenience and comfort, there are additional requirements a good clinical electrode has to meet.
An ideal dry EEG headset should stay on the patient’s head for hours to days or even weeks or more to ensure uninterrupted monitoring of the brain’s electrical activity.
To achieve this in clinical practice, EEG technicians glue the electrodes one by one to the skin with a collodion adhesive, apply the gel and cover the electrodes with a gauze bandage. The drawback of this method is that the gel dries quickly and needs to be replaced every few hours, which requires a trained EEG technologist to do as the head bandage needs to be replaced too.
Therefore, while this type of traditional wet electrode system is acceptable in the clinical settings where EEG technologists are available around the clock, this dependency on skilled labor makes EEG underutilized in many clinical areas, such as ICU, ED, NICU, and stroke centers, to name a few.
In contrast, dry electrode systems do not require an EEG technologist’s assistance to replace the electrodes. Introducing dry electrodes to clinical EEG monitoring, including long-term EEG, would not only free up the time of EEG technologists for EEG monitoring and allow them to complete more EEG studies but would also expand the use of EEG in clinical areas and clinics lacking EEG specialists on site.
Acceptance of the dry electrode systems in the clinical EEG market
Although dry electrode EEG headset systems have multiple advantages over gel-based electrodes, there is a barrier to widespread acceptance.
According to conventional wisdom, the lower the impedance of electrodes the better the quality of the recording is. However, recent technological advances have brought about a new generation of amplifiers capable of amplifying the signal orders of magnitude better than conventional systems and overcoming the impedance-gap of dry electrodes.
In addition, the introduction of active electrode technology, i.e. giving the EEG signal more strength by pre-amplifying the signal close to the electrode, ensures that the biological signal will not be affected by external electromagnetic noise before reaching the second amplifier stage. Conventional EEGs use passive electrodes, which makes the few micro-volt magnitude signals traveling in long cables from the electrode to the amplifier susceptible to electromagnetic noise especially upon movement of the cables.
Moreover, the active electrodes technology applies a driven current to each electrode that is being modulated by the brain’s electrical activity. The modulated signal will be detected by the electrodes and transferred to the amplifiers where the driven current will be subtracted from the signal to recover the brain’s original signal.
In addition to active electrode technology, dry electrode systems need good noise shielding and noise cancellation. As the biosignal travels through ‘unprepared’, high impedance skin layer, it becomes vulnerable to external noise such as 60Hz lines noise or other electrical interference in the room. Hence excellent shielding mechanisms are needed to protect the electrodes.
Moreover, the system needs to incorporate dynamic common mode noise rejection circuitry to improve CMRR (Common Mode Rejection Ratio) above 130dB which allows signal quality to be on par with traditional wet EEG systems.
The Benefits of Dry EEG Headsets
The combination of these technologies makes dry electrodes not only on a par with conventional electrode recording quality but able to exceed that.
As of today, many well-controlled and peer-reviewed studies have proven that dry electrode EEG headset systems are non-inferior to the conventional EEG and they are rapidly improving (Guger, Krausz, Allison, & Edlinger, 2012) (Di Flumeri et al., 2019; Fiedler et al., 2014; Hinrichs et al., 2020; Kam et al., 2019; Leach, Chung, Tüshaus, Huber, & Karlen, 2020; Li, Wu, Xia, He, & Jin, 2020; Mathewson, Harrison, & Kizuk, 2017; Schwarz, Escolano, Montesano, & Müller-Putz, 2020; Shad, Molinas, & Ytterdal, 2020; Zander et al., 2011).
The complicated nature of wet EEGs means they’re limited in the number of people they can reach. Extensive prep is needed, and this requires EEG technologists on hand at every step of the way. This limitation means EEGs can’t be rolled out in many settings where they can be most useful (ICU, ED, NICU, stroke centers, etc).
Dry EEG headsets solve this problem by making the setup simple. The average prep time is just five minutes, and the headset is comfortable for the patient, with gentle support pads making the process much more pleasant.
Of course, this wouldn’t be useful unless the results were accurate, and this is where the hard work has gone on behind the scenes. With technological improvements, studies are showing that results from EEG headsets are on par with conventional EEGs.
By combining accurate results with much-improved convenience, dry EEG headsets represent a great step forward in the way we can study the brain.
Zeto Wireless EEG Headset
The Zeto wireless EEG headset is the first FDA-approved true dry electrode EEG system.
Traditional EEG systems have clear drawbacks, and many hospitals and clinics have been eagerly awaiting a better EEG testing option. That options arrived in 2020, as Zeto’s EEG headset brought new levels of convenience combined with exceptionally accurate results.
The headset offers:
Wireless, battery-powered
No skin-prep, no cleanup
Comfortable, no residue, soft tip electrodes
Adjustable headset for child to adult sizes
Precision placement as per 10-20 system
Easy to learn for anyone familiar with EEG
Live remote viewing of video EEG can be accessed through the cloud allowing for seamless data management, and a mobile EEG system.
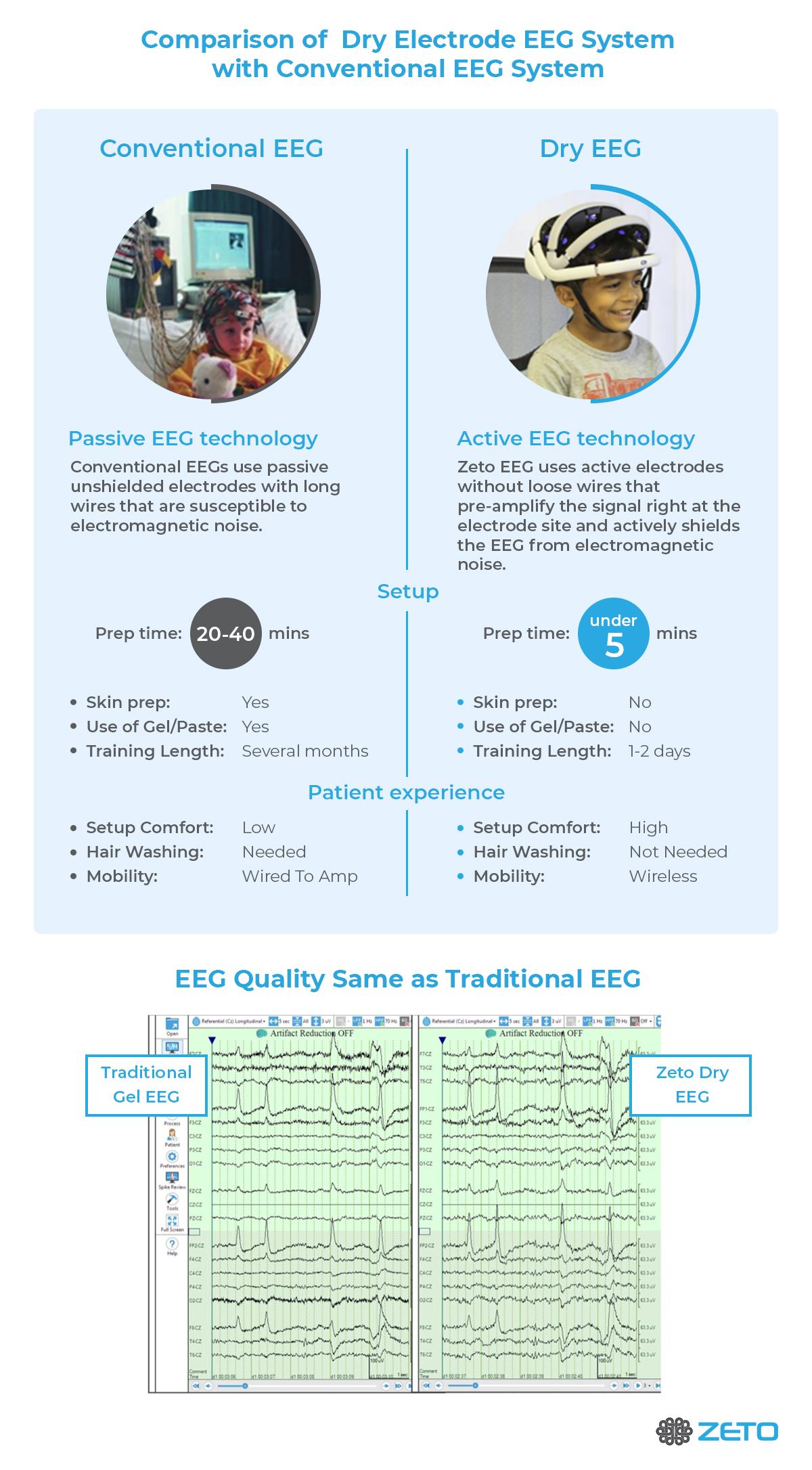
Infographic – Comparison of Dry Electrode EEG System with Conventional System
References
Di Flumeri, G., Aricò, P., Borghini, G., Sciaraffa, N., Di Florio, A., & Babiloni, F. (2019). The Dry Revolution: Evaluation of Three Different EEG Dry Electrode Types in Terms of Signal Spectral Features, Mental States Classification and Usability. Sensors (Basel, Switzerland), 19(6), 1365. https://doi.org/10.3390/s19061365
Fiedler, P., Haueisen, J., Jannek, D., Griebel, S., Zentner, L., Vaz, F., & Fonseca, C. (2014). Comparison of three types of dry electrodes for electroencephalography. In Acta IMEKO. https://doi.org/10.21014/acta_imeko.v3i3.94
Guger, C., Krausz, G., Allison, B., & Edlinger, G. (2012). Comparison of Dry and Gel Based Electrodes for P300 Brain–Computer Interfaces. Frontiers in Neuroscience, 6, 60. https://doi.org/10.3389/fnins.2012.00060
Hinrichs, H., Scholz, M., Baum, A. K., Kam, J. W. Y., Knight, R. T., & Heinze, H. J. (2020). Comparison between a wireless dry electrode EEG system with a conventional wired wet electrode EEG system for clinical applications. Scientific Reports. https://doi.org/10.1038/s41598-020-62154-0
Kam, J. W. Y., Griffin, S., Shen, A., Patel, S., Hinrichs, H., Heinze, H.-J., … Knight, R. T. (2019). Systematic comparison between a wireless EEG system with dry electrodes and a wired EEG system with wet electrodes. NeuroImage, 184, 119–129. https://doi.org/10.1016/j.neuroimage.2018.09.012
Leach, S., Chung, K., Tüshaus, L., Huber, R., & Karlen, W. (2020). A Protocol for Comparing Dry and Wet EEG Electrodes During Sleep. Frontiers in Neuroscience, 14, 586. https://doi.org/10.3389/fnins.2020.00586
Li, G.-L., Wu, J.-T., Xia, Y.-H., He, Q.-G., & Jin, H.-G. (2020). Review of semi-dry electrodes for EEG recording. Journal of Neural Engineering, 17(5), 51004. https://doi.org/10.1088/1741-2552/abbd50
Mathewson, K. E., Harrison, T. J. L., & Kizuk, S. A. D. (2017). High and dry? Comparing active dry EEG electrodes to active and passive wet electrodes. Psychophysiology, 54(1), 74–82. https://doi.org/10.1111/psyp.12536
Schwarz, A., Escolano, C., Montesano, L., & Müller-Putz, G. R. (2020). Analyzing and Decoding Natural Reach-and-Grasp Actions Using Gel, Water and Dry EEG Systems. Frontiers in Neuroscience, 14, 849. https://doi.org/10.3389/fnins.2020.00849
Shad, E. H. T., Molinas, M., & Ytterdal, T. (2020). Impedance and Noise of Passive and Active Dry EEG Electrodes: A Review. IEEE Sensors Journal, 20(24), 14565–14577. https://doi.org/10.1109/JSEN.2020.3012394
Zander, T., Lehne, M., Ihme, K., Jatzev, S., Correia, J., Kothe, C., … Nijboer, F. (2011). A Dry EEG-System for Scientific Research and Brain–Computer Interfaces. Frontiers in Neuroscience, 5, 53. https://doi.org/10.3389/fnins.2011.00053
Every machine requires some circuitry or motherboard that controls the machine’s functions and operations. Likewise, humans also possess a complex computing system inside the body: the brain. The brain’s inner workings and connections are mysterious. An intricate system of neurons link together to form the brain’s jelly-like morphology.
Advancements in medical science and inventions have improved our understanding of how the brain works. One such invention was electroencephalography, a method and device used to record and analyze the electrical activity occurring inside the brain.
While the first EEG was performed in 1924, the technology is constantly evolving. Today, modern portable EEG devices are changing the way we look at the brain.
In this EEG guide, you’ll learn what an EEG machine is, what an electroencephalography is, how the EEG system operates, and what the various devices are used for.
What is Electroencephalography (EEG)?
Electroencephalography 1, or EEG, is a procedure used to measure and record the electrical activity of the brain in the form of waves. One can monitor the neurophysiological function of the brain while the subject is performing different tasks. Various electrical abnormalities can also be detected with precision.
As we understand the brain better, our EEG technology and the way we interpret the signals of the brain continue to improve. This has led to new ways of performing EEGs, such as wireless EEG systems that allow us to continue to learn the secrets of the brain.
What is an EEG?
Our brain is composed of billions of interconnected neurons. These neurons work by generating electrical potentials in the form of neuronal impulses which travel through the brain. EEG works on the principle of measuring these electrical potentials/voltages generated inside the brain.
What is an EEG Machine?
An EEG machine measures these electrical potentials by recording the differences in voltage between various points using a pair of electrodes. Then, the recorded data is sent to an amplifier.
The amplified data is eventually digitized and displayed on the monitor of the EEG machine as a sequence of voltage values that fluctuate in time. The resulting EEG waveforms from the EEG machine are interpreted to detect signs of abnormality inside the brain.
Parts of an EEG Machine
Essentially, an EEG machine is made up of the following primary device(s):
Electrodes: The electrodes pick up small electrical brainwaves produced by neurons. These are attached to the scalp with a special paste. Modern EEG machines possess a wearable cap with electrodes pre-installed inside the cap.
Amplifiers: As the signals travel from the electrodes through the machine, they run through an amplifier that boosts the incoming signal enough to be displayed on the screen.
Computer Control Module: The amplified signals are processed by a computer.
Display Device: The processed signals are displayed on the screen to be analyzed by the operator. Before the digital monitoring methods became prevalent, waveforms were plotted with a moving pen on rolls of graph paper.3
How is an EEG performed?
An EEG test may be performed either as an outpatient study or as part of your stay in the hospital. Various EEG technology and techniques are used depending on your health condition. Generally, an EEG procedure utilizing EEG technology is done in the following way:
The patient is asked to relax by lying on a bed or sitting in a chair.
Various electrodes (between 16, 20, or more) are attached to the scalp using a special electrolyte paste, or the patient is fitted with a cap containing the electrodes.
The patient is then asked to close their eyes and remain still.
Generally, an EEG technologist performs this procedure, which may take from 20 minutes to 2 hours, not including the electrode prepping.
Longer brain monitoring requires the patient to be admitted to the hospital.4
Modern technology has helped make this process easier in recent years. Today, portable EEG devices offer maximum convenience without compromising the quality of the results.
For the EEG operator, this brings down prep times (it’s easy to put on and adjust, and there’s no messy glue or wires to clean up), and for the patient, this offers increased comfort (the soft support pads are gentle on the skin).
Also known as rapid EEGs, these devices make EEG technology much more accessible, allowing more people to benefit from it. The portable EEG machine sends results to the Zeto app, allowing practitioners to access live results from anywhere.
We’re still working hard to understand the human brain, and many mysteries remain, but with each technological improvement in EEG machines, we take a step closer to solving the puzzle of the human brain. Portable EEG machines allow us to study the brain more efficiently, offering benefits to researchers, practitioners, and patients.
What Does an EEG Measure?
At its most basic, an EEG measures brainwaves. Electrical signals generated by the brain are displayed on the screen in the form of waves that vary in amplitude, phase, and frequency.
Fast Fourier Transform (FFT) and other signal processing techniques convert the incoming signals measured by the EEG into useful information that can aid diagnosis. Brainwaves are categorized into four main types based on frequency: Infra-low, Delta, Theta, Alpha, Beta, and Gamma.
Each brainwave is associated with particular functions of the brain. The following paragraphs discuss the various important functions of the brain in correlation with the types of brainwaves.
Delta Waves (frequency ranging from 0.5 Hz to 3 Hz)
Delta waves are slow but loud brainwaves (like the deeply penetrating waves of a drum beat). They are generated during dreamless sleep. Delta waves are intermittent with sleep spindles and sharp waves. When delta waves synchronize between distant cortical areas, they often trigger sharp waves that are considered to be relevant for memory consolidation. 6
Theta Waves (frequency ranging from 3 Hz to 7 Hz)
Theta waves mostly occur during REM sleep. They derive from deep subcortical sources, making them mostly undetectable with an EEG machine. The predominant occurrence of theta is pathological. Normal theta waves are known to be involved in learning and memory. In theta state, we experience dreams comprising vivid imageries and intuitions. 7
Alpha Waves (frequency ranging from 7 Hz to 13 Hz)
Alpha waves occur when the person is in a relaxed, lucid, or calm state. These are mostly found in the occipital and posterior regions of the brain. Whenever someone is asked to close his/her eyes and then relax, the brain is disengaged from any complex cognitive tasks or thinking, and alpha waves are induced. 8
Beta Waves (frequency ranging from 14 Hz to about 38 Hz)
Beta waves refer to the alert, attentive, and conscious state of mind. These are of low amplitude and are also associated with motor decisions. Beta waves are further subdivided into:
Low-Beta Waves (Beta1, 12-15 Hz): occur while musing
Mid-Beta Waves (Beta2, 15-22 Hz): occur while engaging intensely in something or actively figuring something out.
High-Beta Waves (Beta3, 22-38 Hz): occur during complex thoughts and integration of new experiences. Also related to severe anxiety or excitement. 9
Gamma Waves (frequency ranging from 38 Hz to 120 Hz)
These are the fastest of all the brainwaves with the highest frequency and smallest amplitude. Because of the small amplitude and high frequency, they are often contaminated by electrical noise or muscle artifacts.
If gamma waves are captured and measured by EEG, they inform us about information processing in the brain.10 The synchrony of gamma waves between different parts of the brain reflects information exchange between those areas. Gamma waves still remain a mystery as these waves orchestrate the synchronized activity of neurons.
Low-Gamma Waves (38-60 Hz): Active attentive behavior and cognitive tasks
High-Gamma Waves (60-120 Hz): Their function is not quite clear, but the predominant occurrence is regarded as diagnostic of epilepsy.
What Does an EEG Test Diagnose?
EEG technology is currently used to diagnose and help treat brain-related disorders.
EEG is the most powerful and preferred diagnostic procedure for epilepsy.13
EEG is very helpful in diagnosing sleep disorders such as insomnias, parasomnias, etc.14
EEG has valuable diagnostic potential for other neurological conditions such as Stroke, Autism, Depression, and ADHD, to name a few.
EEG is turning out to be the tool for the next generation of Brain-Computer Interfaces and Neural Prosthetics
EEG can be used to track attention during several activities, to help design strategies to reduce stress and improve focus.15
EEG has been introduced as a new tool for Neuromarketing studies to help objectively identify participants’ responses.
And the list is growing…
The Bottom Line
The invention of the EEG system opened a new window of learning about the brain. With the EEG system to guide them, neurologists have been able to successfully treat seizures, epilepsy, sleep disorders, and other neurological issues.
As EEG becomes simpler, easier to acquire and interpret, and wireless, even more can be achieved. With new advancements in electronics, cloud computing, and machine learning, it is just a question of how soon.
The future of EEG is bright. Consequently, the advancements in our understanding of the brain cannot be more exciting. Learn more about wet vs. dry EEG tests here.
2. Introduction – Electroencephalography (EEG): An Introductory Text and Atlas of Normal and Abnormal Findings in Adults, Children, and Infants – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK390346/.
3. Wang, C. S. Design of a 32-channel EEG system for brain control interface applications. J. Biomed. Biotechnol.2012, (2012).
4. Light, G. A. et al. Electroencephalography (EEG) and event-related potentials (ERPs) with human participants. Current Protocols in Neuroscience vol. CHAPTER Unit (2010).
5. Watson, B. O. Cognitive and physiologic impacts of the infraslow oscillation. Frontiers in Systems Neuroscience vol. 12 44 (2018).
6. Harmony, T. The functional significance of delta oscillations in cognitive processing. Frontiers in Integrative Neuroscience vol. 7 (2013).
7. Zhang, H. & Jacobs, J. Traveling theta waves in the human hippocampus. J. Neurosci. 35, 12477-12487 (2015).
8. Klimesch, W. Alpha-band oscillations, attention, and controlled access to stored information. Trends in Cognitive Sciences vol. 16 606-617 (2012).
11. Michal T. Kucewicz, Brent M. Berry, Vaclav Kremen, Benjamin H. Brinkmann, Michael R. Sperling, Barbara C. Jobst, Robert E. Gross, Bradley Lega, Sameer A. Sheth, Joel M. Stein, Sandthitsu R. Das, Richard Gorniak, S. Matthew Stead, Daniel S. Rizzuto, Michael J. Kahana, Gregory A. Worrell, Dissecting gamma frequency activity during human memory processing, Brain , Volume 140, Issue 5, May 2017, Pages 1337-1350, https://doi.org/10.1093/brain/awx043
12. Ren, L., Kucewicz, M. T., Cimbalnik, J., Matsumoto, J. Y., Brinkmann, B. H., Hu, W., Marsh, W. R., Meyer, F. B., Stead, S. M., & Worrell, G. A. (2015). Gamma oscillations precede interictal epileptiform spikes in the seizure onset zone. Neurology , 84 (6), 602-608. https://doi.org/10.1212/WNL.0000000000001234
13. Smith, S. J. M. EEG in the diagnosis, classification, and management of patients with epilepsy. Neurology in Practice vol. 76 2-7 (2005).
14. Tan, D. E. B., Tung, R. S., Leong, W. Y. & Than, J. C. M. Sleep disorder detection and identification. in Procedia Engineering vol. 41 289-295 (Elsevier Ltd, 2012).
15. Thompson, T., Steffert, T., Ros, T., Leach, J. & Gruzelier, J. EEG applications for sport and performance. Methods 45 , 279-288 (2008).






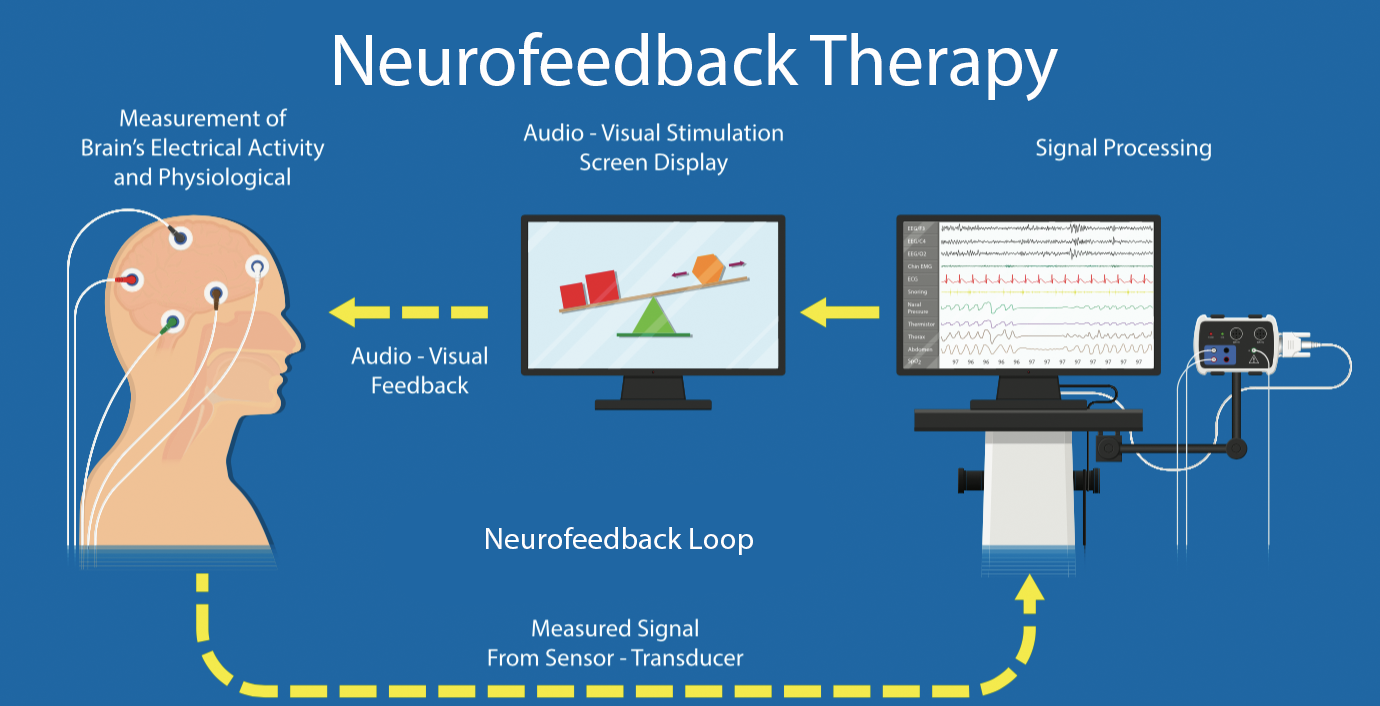
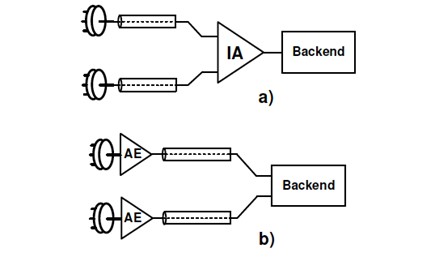
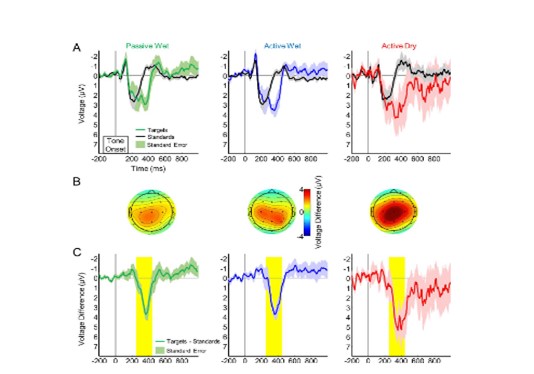 Source |
Source |